- Health
Inadequate analysis of Japan data used to spread false claim about COVID-19 vaccine mortality
Key takeaway
When comparing an unvaccinated group with a vaccinated group, it is important to ensure that the two are similar to each other in terms of variables like age and underlying medical conditions, as these variables can influence outcomes that are examined in a study, like mortality. COVID-19 vaccines help reduce the risk of complications and death from COVID-19. Multiple published studies have shown that COVID-19 vaccination isn’t associated with a higher risk of mortality.
Reviewed content

Verdict:
Claim:
Japanese database of 18 million vaccinated people show that the more COVID-19 vaccine doses you get, the sooner you die
Verdict detail
Misleading:
Published studies haven’t found an association between COVID-19 vaccination and higher mortality. The analysis presented by a Japanese activist group didn’t account for potential differences in age and underlying medical conditions between unvaccinated and vaccinated groups, which could have skewed results and led to invalid conclusions.
Factually inaccurate:
The database contained records linked to 18 million vaccine doses, not 18 million people.
Full Claim
“Japanese doctors with a database of 18 million vaccinated people have found: the more shots you get, the sooner you die.”; “Japan Releases Bombshell Vax vs. Unvax Data on 18 Million People”
Review
In June and July 2025, social media posts claimed a Japanese database of 18 million vaccinated people showed that the more COVID-19 vaccine doses received, the sooner a person would die. The claim was posted by accounts on X with large follower counts such as former Newsmax correspondent Emerald Robinson and political activist Peter Imanuelsen (aka Peter Sweden). Altogether, the claim received more than a million views on X.
It was also disseminated by outlets with a history of publishing vaccine misinformation like InfoWars and Slay News. We wrote about Slay News and its use of AI-generated personas in detail before.
Science Feedback explained in previous reviews that COVID-19 vaccination isn’t causally associated with a higher mortality rate. In this review, we will explain why the Japanese analysis in question is inadequate and show that published studies employing more rigorous methods haven’t found an association between COVID-19 vaccination and higher mortality.
Claim based on data presented by mRNA vaccine opponents, not peer-reviewed
The claim originates from videos livestreamed by Japanese activist group United Citizens for Stopping mRNA Vaccines. The group posted a livestream in Japanese in June 2025, while one in English was posted in July 2025. Note that the data hasn’t been published in a peer-reviewed journal.
These videos shared data obtained through Freedom of Information requests made by the group to various municipalities in Japan. The data was also made publicly available online.
Both the Japanese and English livestreams were hosted by journalist Masako Ganaha, a member of United Citizens for Stopping mRNA Vaccines, and the data was presented by Yasufumi Murakami, a professor emeritus at Tokyo University of Science. Murakami is also a member of the International Medical Alliance, formerly the Front Line COVID-19 Critical Care Alliance, a group that spread misinformation about COVID-19 treatments and vaccines.
Other participants in the English livestream were Mike Adams, founder of NaturalNews, a network of websites disseminating misinformation about health, and Dutch anti-COVID vaccine activist Willem Engel.
French fact-checking group Les Surligneurs noted that the group behind the database later issued a correction on X (in Japanese), stating that their data was actually vaccination records for 18 million vaccine doses, not 18 million people. Therefore, claims that the database was for 18 million vaccinated people are inaccurate in this regard.
In addition, the livestream referenced a Danish analysis that allegedly showed a difference in post-vaccination mortality based on vaccine lots. Science Feedback reported on the analysis in a previous review and showed that its method was flawed and its conclusions inaccurate.
The English and Japanese livestreams discussed the same data, but for the purpose of this review, we will discuss content as it was presented in the English livestream.
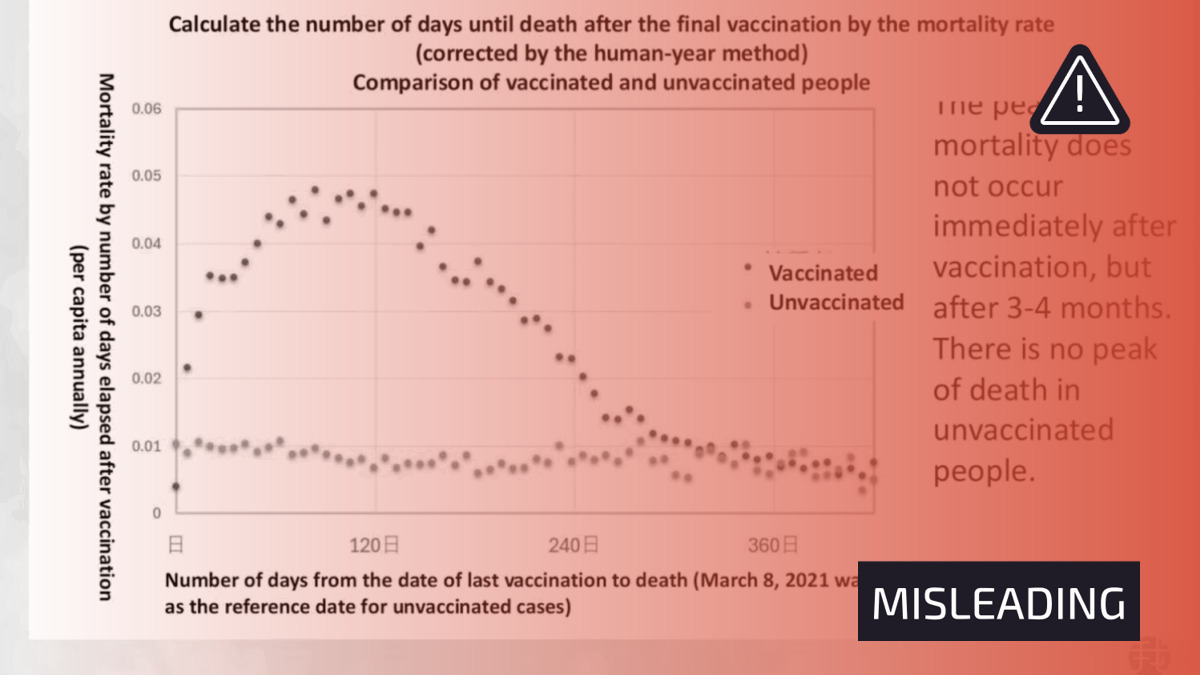
During the livestream, Murakami presented a few graphs. One compared the mortality rate in a vaccinated population post-vaccination with that of the unvaccinated population (see Figure 1 below). This graph showed a peak in mortality roughly three to four months after the last vaccine dose. Murakami claimed that “If the vaccine does not induce death, then such a peak should not be visible”.
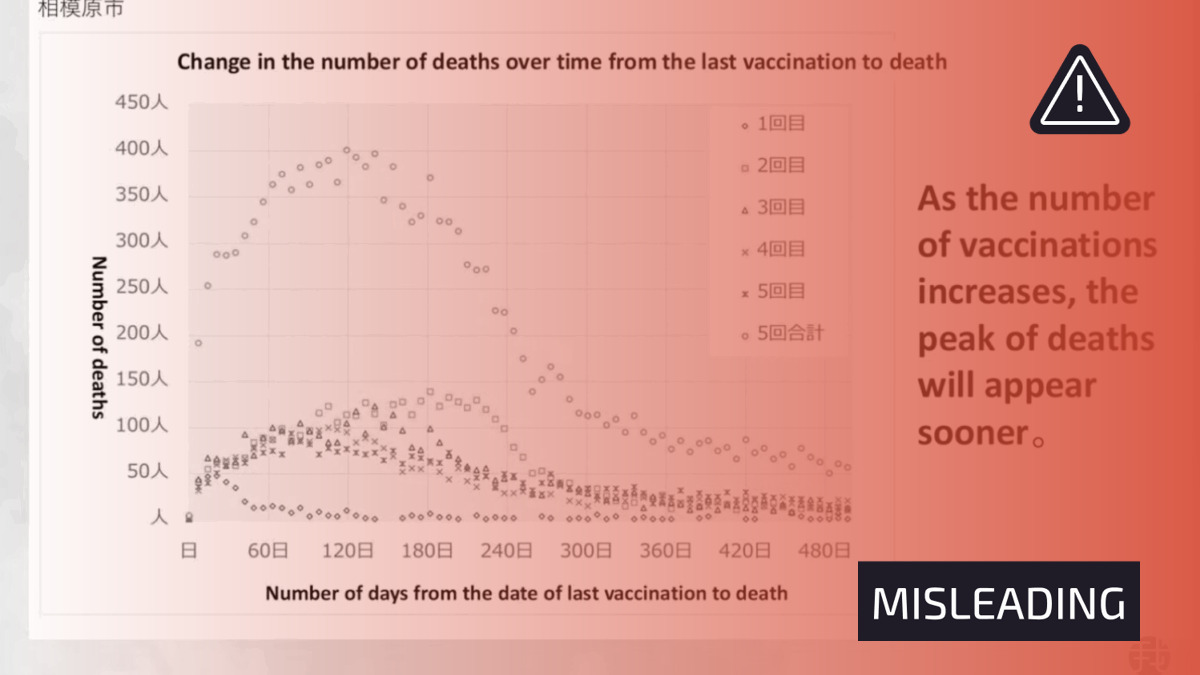
Another graph showed the number of deaths over time for groups receiving differing amounts of vaccine doses (see Figure 2 below). Here, Murakami claimed that “it is clear that as the number of vaccinations increases”, the sooner death occurred.
Both graphs form the basis for the claim reviewed. However, neither are credible evidence for the claim. We explain why below.
Analysis didn’t account for potential difference in age between unvaccinated and vaccinated groups
While Figure 1 showed a peak in mortality rate in the vaccinated group, this correlation alone isn’t sufficient to establish a causal association between the vaccines and post-vaccination deaths. It’s also worth noting the Japanese database itself cautions that the data doesn’t indicate the cause of death or allow one to establish a connection between death and the vaccine.
The approach used in these graphs also doesn’t allow one to rule out the effect of confounding factors. Confounding factors are variables that influence the results of an experiment but aren’t the variables being studied in the experiment. One problem with confounding factors is that they can create the appearance of an association between two variables that doesn’t actually exist. Therefore, studies need to account for confounding factors in order to mitigate bias. Otherwise the risk of arriving at incorrect conclusions is high.
But this wasn’t done with the data presented in the graphs. For instance, no information was provided about the demographics of the vaccinated group. This information is important because people at an advanced age and who have certain underlying medical conditions have a higher rate of mortality, including from COVID-19, compared to younger people.
It’s unclear where data about unvaccinated people in Figure 1 came from, but if the unvaccinated group generally tended to be younger and healthier compared to the vaccinated group, this could explain the lower mortality rate in the unvaccinated group.
In a post on X, Jeffrey Morris, a professor of biostatistics at the University of Pennsylvania, commented on the analysis, stating that “The claim is based on misinterpretation and failure to adjust for obvious age confounding”.
Failure to account for various confounding factors when comparing mortality in unvaccinated and vaccinated populations has been a common feature in COVID-19 vaccine misinformation, as we discussed extensively in a previous Insight article.
Analysis didn’t demonstrate “the more shots you get, the sooner you die”
The conclusion that Figure 2 shows getting more doses means a quicker death isn’t supported by the data presented. While Figure 2 does show that the most number of deaths occurred in the group receiving five doses, there appears to be no clear difference or pattern in the timing of deaths between the groups. No statistical analysis was presented during the livestream showing that there was a meaningful difference in the time of deaths based on vaccine doses received.
If it’s true that “the more shots you get, the sooner you die”, then we would expect to see an incremental effect on the timing of deaths as the number of doses received increases (dose-dependent effect). But this isn’t the case, so the conclusion is inconsistent with the data.
It’s also important to account for vaccine recommendation policies here. Japan’s Ministry for Health, Labour, and Welfare states that “People aged 65 and older, those with underlying medical conditions and health care workers will be vaccinated twice a year while the others once a year. Vaccinations remain free of charge […] This vaccination program continues until March 2024”.
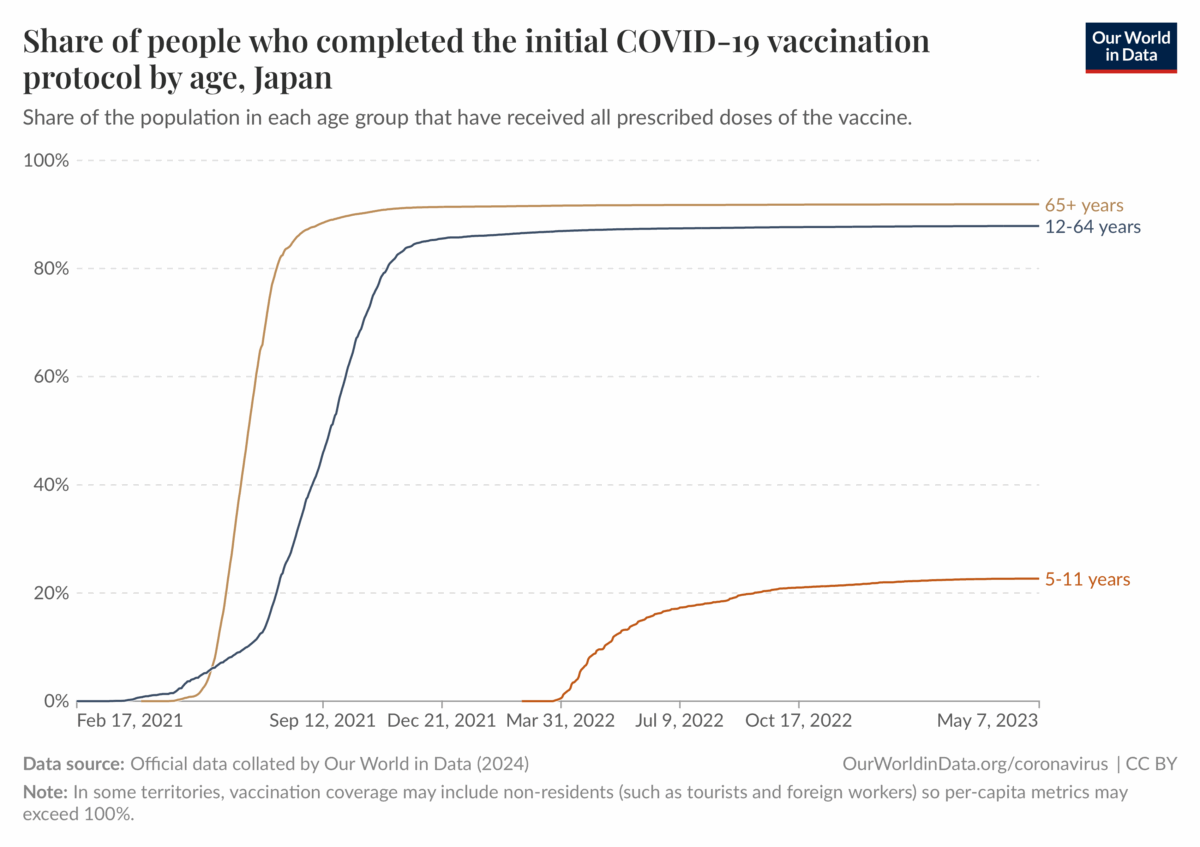
Data up to May 2023 shows that the vast majority of the Japanese population completed the primary vaccine series (Figure 3 below).
However, uptake of a third booster dose was lower, hovering below 70% for the group aged 12 to 64 (Figure 4 below). Booster uptake was highest in the group aged 65 and above.
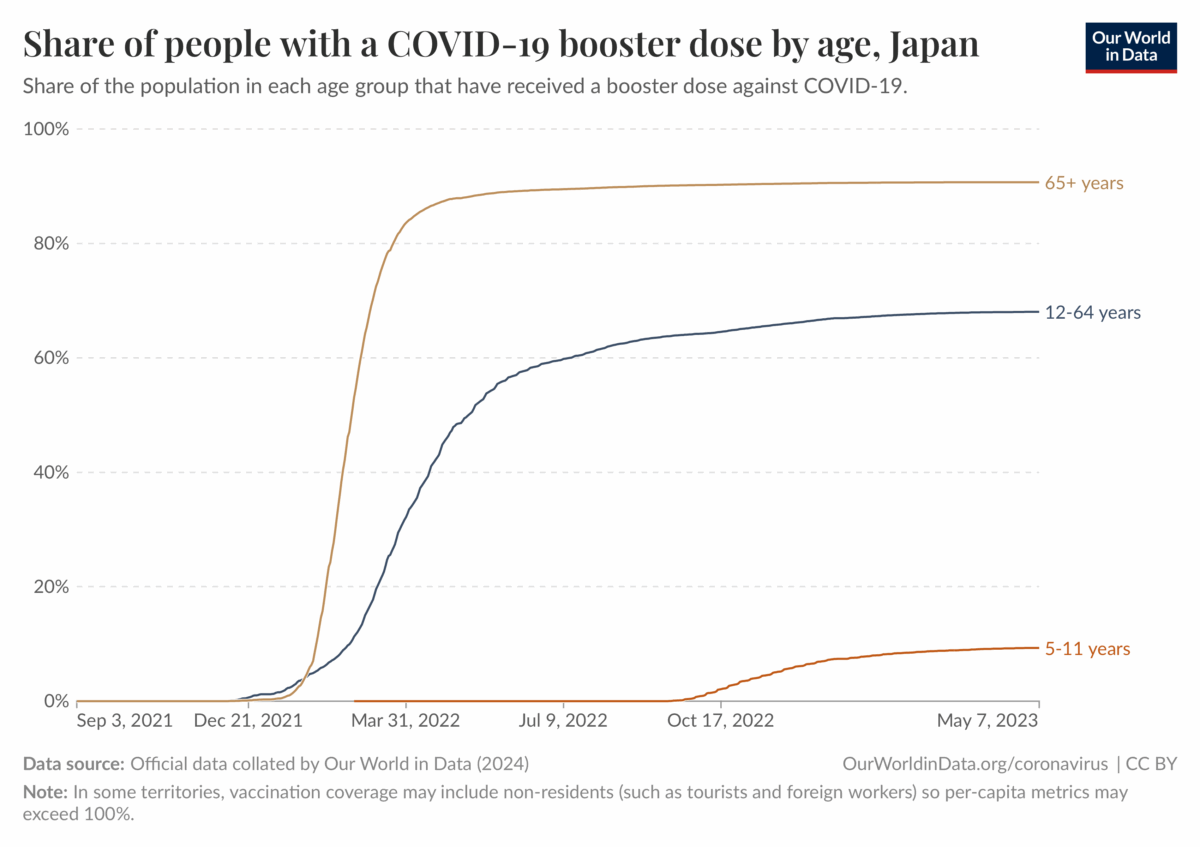
When taken together, this information suggests that the group that received five doses is likely an outlier that isn’t representative of the general population. This group could include a greater proportion of people with underlying medical conditions and the elderly. These populations are likely to have a higher mortality rate than the general population, which could have contributed to the higher mortality seen in Figure 2.
There are also other issues with the data analysis. For example, unlike Figure 1, it didn’t account for the size of each group by expressing mortality as a proportion of the number of people (e.g. deaths per 100,000 people). The reason for this is unclear. All other things being equal, larger groups tend to have more deaths than smaller groups, even if their mortality rate is the same. This means that seeing more deaths in a larger group compared to a smaller group doesn’t automatically indicate the larger group is more prone to dying.
Finally, on the top-left hand corner of Figure 2, the word “Sagamihara” in Japanese can be seen. Sagamihara is a city in Kanagawa Prefecture. This suggests that the data shown in that graph is specific to that area. No reason was given in the English livestream as to why this area should be the sole focus of this analysis.
In summary, the way in which the data was analyzed and interpreted is misleading and incorrect. There’s no indication the analysis ensured that the groups being compared were similar to each other or that it accounted for important confounding factors like age and underlying medical conditions.
Science Feedback reached out to Murakami for comment, but didn’t receive a response by the time of publication.
Published studies didn’t find an association between COVID-19 vaccination and all-cause mortality
The claims made in the livestreams aren’t corroborated by published studies that did account for various confounding factors. These studies didn’t find COVID-19 vaccination to be associated with a higher risk of death[1-4].
There is no medical intervention that exists that carries no risk, and COVID-19 vaccines are no exception. However, the risks posed by the vaccine aren’t equivalent to that posed by the disease. While COVID-19 mRNA vaccines are associated with a risk of myocarditis, mainly in young males, this risk is smaller than that from COVID-19. COVID-19 also increases the risk of various complications like blood clots, heart problems, and neurological problems.
Getting vaccinated, on the other hand, mitigates the risks associated with COVID-19. On balance, the benefits of getting vaccinated outweigh the risks of the vaccine.
Conclusion
When investigating a potential association between two variables, it is important to account for confounding factors because they can create the appearance of an association that isn’t real. This can lead to incorrect conclusions. Ensuring that the groups being compared in an analysis are similar to each other also helps to mitigate the risk of arriving at incorrect conclusions. COVID-19 vaccines help reduce the risk of complications and death from COVID-19. Multiple published studies have shown that COVID-19 vaccination isn’t associated with a higher risk of mortality.
References:
- 1 – Xu et al. (2021) COVID-19 Vaccination and Non–COVID-19 Mortality Risk — Seven Integrated Health Care Organizations, United States, December 14, 2020–July 31, 2021. Morbidity and Mortality Weekly Report.
- 2 – Liu et al. (2023) Effectiveness of COVID-19 vaccination against COVID-19 specific and all-cause mortality in older Australians: a population based study. The Lancet Regional Health Western Pacific.
- 3 – Bilinski et al. (2023) COVID-19 and Excess All-Cause Mortality in the US and 20 Comparison Countries, June 2021-March 2022. JAMA Network.
- 4 – Tu et al. (2023) SARS-CoV-2 Infection, Hospitalization, and Death in Vaccinated and Infected Individuals by Age Groups in Indiana, 2021‒2022. American Journal of Public Health.


