- Health
South Korea study isn’t evidence that COVID-19 vaccines cause cancer
Key takeaway
Claims that unvaccinated people are more healthy than vaccinated people tend to rely on flawed comparisons. A common issue with these comparisons is that they don’t account for important differences between the two groups that change the likelihood of disease detection, such as attitudes towards mainstream medical care and health-seeking behaviour. Finding more diagnoses in one group doesn’t necessarily mean that group is more likely to be ill; it could also mean that diseases are just more likely to be detected in that group. Likelihood of detection is not the same thing as the risk of disease.
Reviewed content

Verdict:
Claim:
South Korea study shows COVID-19 vaccines increase the risk of cancer
Verdict detail
Inadequate support:
The South Korea study contained numerous methodological problems that undermine the validity of its results. As such, it doesn’t provide reliable evidence for a causal relationship between COVID-19 vaccines and cancer risk.
Misleading:
The study reported an association between COVID-19 vaccination and an increased risk in certain types of cancer, but association alone isn’t evidence of causation.
Full Claim
“COVID-19 ‘Vaccines’ Increase Your Risk of SEVEN Cancer Types”; “All COVID Vaccines Increase Cancer Risk, New Study Concludes”
Review
In October 2025, numerous social media posts claimed that a study from South Korea showed COVID-19 vaccines increase the risk of cancer.
Some posts came from individuals with a record of spreading COVID-19 vaccine misinformation. Among them were John Campbell, a retired nurse educator, who posted a YouTube video containing the claim, which was viewed more than 140,000 times. Epidemiologist Nicolas Hulscher, who co-authored a flawed analysis used to claim that a majority of deaths in vaccinated people were due to the vaccine, made a similar post on X. The anti-vaccine organization Children’s Health Defense also published an article with the headline “All COVID Vaccines Increase Cancer Risk”.
This claim isn’t new; past reviews from Science Feedback covered various iterations of the claim (see here, here, and here). As our reviews show, these typically rely on methodologically flawed analyses as supporting evidence.
The latest iteration is based on a study published on 26 September 2025, which examined the health insurance records of more than eight million people in South Korea between 2021 and 2023[1]. Like previous variations of this claim, the study contains significant methodological shortcomings that undermine the validity of its results and conclusions.
In this review, we discuss the background of the study, explain its methodological issues and why it doesn’t show a causal relationship between COVID-19 vaccination and cancer.
Where was the study published and how was it done?
The study appeared in the peer-reviewed journal Biomarker Research, lending the study a degree of scientific credibility. While peer review is important, the process isn’t perfect and just because a study has been peer-reviewed doesn’t necessarily mean it is beyond reproach, as Andrew Wakefield’s now-discredited study and the Surgisphere scandal during the COVID-19 pandemic demonstrated all too well. It’s also important to note that the journal added a notice to the study on 22 October, citing “concerns with this article [that] have been raised with the Editors”.
The study aimed to explore whether COVID-19 vaccines could alter the risk of different types of cancer. To do this, it examined data from the Korean National Health Insurance database for more than eight million people from January 2021 to 31 December 2023.
The outcomes evaluated in the study were cancer diagnoses at different points in time after vaccination: specifically, one, three, six, and nine months, and a year post-vaccination. This type of research study, which examines outcomes after exposure to a potential risk factor, is also called a retrospective cohort study.
Roughly 2.3 million vaccinated people and 595,000 unvaccinated people were included in the study. In their analysis, the authors accounted for variables like age, sex, insurance coverage (a proxy for socioeconomic status), preexisting medical conditions, and COVID-19 risk factors. This is important since these variables, also known as confounding factors, can influence a person’s cancer risk independent of the variable of interest (in this case, the COVID-19 vaccines). Failing to account for the effect of confounding factors can lead to erroneous conclusions.
The majority of vaccinated people received the Pfizer-BioNTech COVID-19 mRNA vaccine as the first (67%) and second (74%) doses. The rest received a viral vector COVID-19 vaccine—the authors didn’t specify which brands, but given the time frame of the study, it could have been the AstraZeneca or Janssen vaccine, both of which were authorized in South Korea. About 62% of vaccinated people went on to receive a third dose (booster), almost all of which were mRNA vaccines.
Important methodological shortcomings in the study
Science Feedback reached out to Dan Chaltiel, an epidemiologist and biostatistician at the Gustave Roussy Institute and the Centre de recherche en épidémiologie et santé des populations (Center for Research in Epidemiology and Population Health), to analyze the study’s methods and findings.
Immortal time bias
Chaltiel highlighted one major issue with the study, which is “immortal time bias”:
“In the study, the vaccinated were enrolled into the study based on the date of their last dose, while all the unvaccinated were enrolled on a fixed date (1 January 2022). The study period began on 1 January 2021. This means that an unvaccinated person who was diagnosed with cancer in 2021 would be excluded from the study, while a vaccinated person who had their first dose in 2021 and was diagnosed with cancer shortly after vaccination would be included in the study. This results in fewer cancer diagnoses being counted in unvaccinated people. This bias alone is sufficient to explain the results, without invoking a supposedly carcinogenic effect from the vaccines.”
This bias arises because the eligibility criteria for vaccinated and unvaccinated people to be included in the study were different. Unvaccinated people already diagnosed with cancer prior to 1 January 2022 would have been entirely excluded from the study as a rule, but vaccinated people were included on the basis of their vaccination date, which could precede 1 January 2022. If a person was diagnosed with cancer in 2021 after vaccination, their diagnosis would be recorded, but the same diagnosis for an unvaccinated person in 2021 would be left out.
The end result is that more cancer diagnoses are counted in the vaccinated group, simply because more time from that group was included in the study.
As epidemiologist Ellie Murray wrote in her blog post, “[A]sk yourself ‘when can the outcome happen?’. If the answer is ‘any time at all’ for one group and ‘only after eligibility’ for the other group, then there’s a risk of immortal time bias”.
Surveillance bias
A fair comparison between a control group and a treatment group requires both groups to be as similar to each other as possible, so that any difference seen in the groups can reliably be attributed to the treatment. But we can infer from the study’s characteristics that this was unlikely to be the case. Chaltiel pointed out the following:
“The study population chosen by the authors comprised 7,700,000 vaccinated people and just 680,000 unvaccinated people, which is 8% of the study population. We can deduce that the unvaccinated group is very much an outlier and that the characteristics of this group make them non-comparable to the vaccinated group.
For example, if the unvaccinated are highly skeptical of mainstream medical care, which is often the case in Europe, they go to the doctor less often and will therefore receive fewer cancer diagnoses. This is what we call ‘surveillance bias’: the unvaccinated always receive fewer diagnoses than the vaccinated (or receive them at a later stage), even if they are just as likely to become ill.”
The authors of the study also recognized this drawback in their study, stating in the Supplementary Material of the study:
“For the surveillance issue, there may be systematic differences in health surveillance intensity between the two groups. However, given South Korea’s single-payer healthcare system and its high accessibility, individuals generally have a uniformly high rate of medical center visits, which may reduce such differences. In addition, the study region (Seoul) is considered one of the most medically accessible areas, further minimizing spatial or socioeconomic inequalities.”
The “uniformly high rate of medical center visits” cited by the authors, however, imply that we can safely assume health-seeking behaviour is similar across the entire study population. But the study provided no data to support this assumption. We reached out to the authors to ask if they had data representing the health-seeking behaviour of the unvaccinated and vaccinated groups, and will update this review if more information becomes available.
No credible biological mechanism to explain carcinogenic effect
The majority of vaccinated people included in the study received a COVID-19 mRNA vaccine. These vaccines work by providing cells with the mRNA template to make the spike protein, which is used to train the immune system so that it can mount an immune defense quickly in the event of a future infection.
Part of the authors’ rationale for their hypothesis is the existence of cancer-causing viruses,, such as the human papillomavirus (which causes cervical cancer as well as cancers affecting the anogenital areas), and the Epstein-Barr virus (which is linked to nasopharyngeal cancer). Furthermore, these viruses make proteins similar to the spike protein. These two observations combined form the basis for the hypothesis that SARS-CoV-2 is a potential carcinogen, which the authors referenced in their study citing this review.
Taking this a step further, the authors proposed that the COVID-19 vaccines could increase cancer risk, since they also entail exposure to the spike protein, though they acknowledged that there is “limited availability of real-world data” showing this.
Since 2020, researchers have been studying the potential effects that the SARS-CoV-2 virus has on the human body at a cellular and molecular level. However, the results so far haven’t uncovered any mechanisms through which either the virus or the vaccines could induce cancer.
Furthermore, most of the world’s population was exposed to SARS-CoV-2, regardless of vaccination status. If the spike protein does cause cancer, we should have seen a sudden and unusual rise in cancer. But in South Korea at least, epidemiological data from 2021 didn’t show such a concerning increase[2].
Cancer doesn’t develop in a year
It’s important to note that cancer typically takes several years to develop. In fact, most cancers, with the exception of blood cancers, have a long latency period, ranging between five to ten years. Some have claimed that COVID-19 vaccines cause “turbo cancer”, or rapidly developing cancers, but this hasn’t been substantiated by the evidence.
The authors acknowledged this caveat in the Supplementary Material, though not in the main text of the study itself:
“Furthermore, as most solid tumours require more than 1 year to develop, our one-year follow-up period is relatively short for evaluating cancer incidence, and the possibility of reverse causation or surveillance bias cannot be excluded.”
David Gorski, a surgical oncologist and editor of Science-Based Medicine, pointed out that even in the case of ionizing radiation, a very powerful carcinogen, it still takes about two years for blood cancers to manifest; in the case of solid tumors, this takes a decade. Add to this the improbability of COVID-19 vaccines being more carcinogenic than ionizing radiation.
The bottom line is that the South Korea study, with its follow-up period of one year post-vaccination, is unlikely to capture cancer-related outcomes that are allegedly the result of vaccination. Instead, the increased risk observed in the study is more likely the result of detection bias, in which vaccinated people are more likely to have their cancers detected.
Other concerns
If COVID-19 vaccines cause cancer, we should expect this risk to be consistently present over time. However, Chaltiel noted that Figure 1B of the study (see below) suggested otherwise. Specifically, the overall incidence of cancer in the vaccinated rose more quickly than in the unvaccinated for the first six months, but after six months, the rate at which cancer incidence increased in both groups became similar, with both lines becoming parallel to each other.
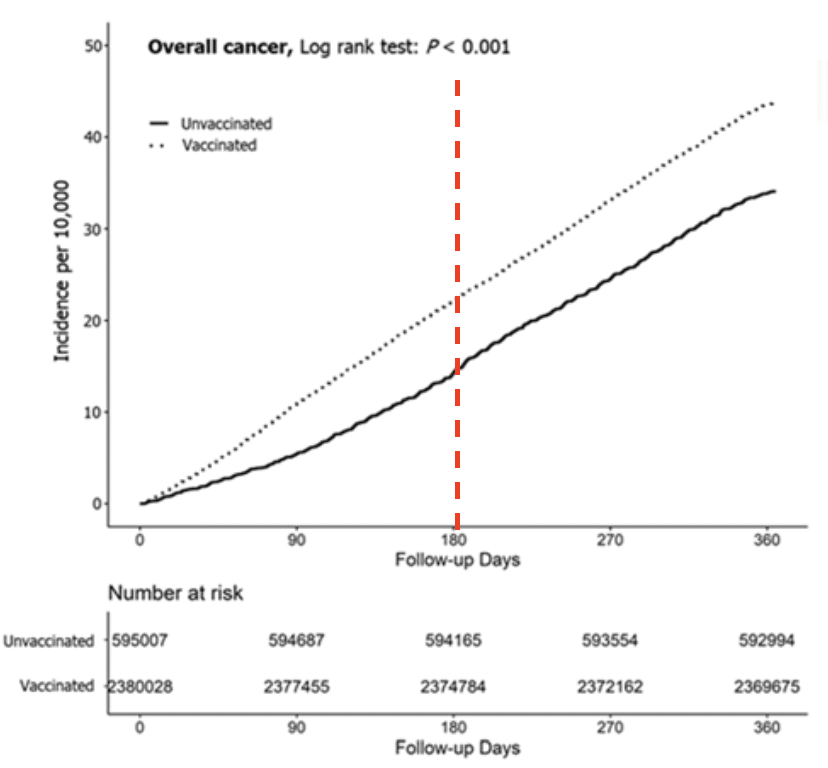
This suggests that cancer risk was only higher in the first six months post-vaccination and this increased risk disappeared afterwards—something that is biologically improbable if the vaccines are truly cancer-causing.
It’s important to note that the authors themselves described their findings as an association between vaccination and cancer, specifically that more cancers were observed in vaccinated people compared to unvaccinated people. But they didn’t report that the vaccines caused cancer.
Scientific research is key to uncovering potential relationships between vaccines and side effects, and improving vaccine safety. However, there are no shortcuts to this endeavor: time and many properly-conducted studies are essential—a single study containing numerous flaws cannot furnish credible evidence of cause-and-effect.
Chaltiel said:
“If the study’s initial hypothesis is well-founded, if there are no evident biases in the study, and if the study appears to be conducted rigorously, then we can infer that a causal relationship might exist. This would call for further studies looking at the same question, using different methods and approaches, and if the findings of these studies are consistent with one another (as in the case of smoking and lung cancer), then a causal relationship is established. But in this instance, the initial hypothesis doesn’t hold up in terms of biological mechanism and there are several concerning biases. If the association found in the study turns out to be causal indeed, it would only be through pure chance, just as a broken clock is right twice a day.”
Conclusion
A South Korea study that examined health insurance data for millions of people reported a higher risk of cancer in people who received the COVID-19 vaccine compared to unvaccinated people. However, the study is founded on the hypothesis that the virus SARS-CoV-2 can provoke cancer in humans, something that remains unproven to date. Furthermore, the study only looked at a period of one year post-vaccination, which is too short for most forms of cancer to have developed.
The study was also conducted in a manner that introduced several biases, notably immortal time bias due to the differences in the way vaccinated and unvaccinated people were included in the study. This bias made it more likely for cancer in unvaccinated people to be missed. This issue was further compounded by surveillance bias, which could artificially suppress detected cancers in unvaccinated people. These methodological shortcomings undermine the validity of the study’s results and conclusions.
Reviewers’ feedback

Dan Chaltiel
Epidemiologist and biostatistician, Institut Gustave Roussy – Centre de recherche en épidémiologie et santé des populations
The following is a translation of the reviewer’s comments, originally published in French.
The time window examined in this study is extremely limited! In general, at least five to six years of follow-up is needed in order to detect outcomes related to cancer, but this study had an average follow-up period of one year. Cancer is an indolent disease that develops over years. To think that an exposure could increase cancer incidence so quickly is an extraordinary hypothesis. It’s possible that this is about a rise in the relapse of preexisting cancers, but this doesn’t appear to be the hypothesis of the authors and in any event, the two effects aren’t the same.
Figure 1B of the study is very unusual. The two curves diverge for six months and then become parallel to each other. This implies that there’s no increased cancer risk linked to vaccination. Biologically speaking, this means that the alleged cancer-causing effect of the vaccine disappears after six months, which is improbable.
It’s here that the main issue with the Cox model used in the study becomes apparent. The increased risk is represented by the hazard ratio (HR), but one of the most important assumptions about the hazard ratio is that it should remain valid over time. The curves [in Figure 1B] show that the hazard ratio is greatly elevated [in the vaccinated] (a three- or fourfold increase in risk for instance) for a few months, and then diminishes almost entirely after six months. These results are condensed in Figure 1A, where the overall hazard ratio is reported to be roughly 1.3.
These observations suggest that the results are highly biased. With a longer follow-up time of five or six years, the initial difference in terms of the rise in cancer incidence between the two groups would count for less and reduce the effect of bias on the results (the overall HR would then be closer to 1).
Another serious issue: in the study, the vaccinated were enrolled in the study based on the date of their last dose, while all the unvaccinated were enrolled on a fixed date (1 January 2022). The study period began on 1 January 2021. This means that an unvaccinated person who was diagnosed with cancer in 2021 would be excluded from the study, while a vaccinated person who had their first dose in 2021 and was diagnosed with cancer shortly afterwards would be included in the study. This results in fewer diagnoses being counted in unvaccinated people. This bias alone is sufficient to explain the results, without invoking a purportedly carcinogenic effect from the vaccines.
Finally, the results obtained from patients who received a third booster dose don’t appear to be robust at all. The authors ran 30 statistical tests, with the assumption of a 5% false-positive rate. There’s no mention of correction for the p-value [a statistical measure of how likely a difference between groups is due to chance alone] #. If we ran our own calculations with a p-value of 0.05, sample size (N) of 30, and number of significant results (x) set at 1 or 3, there is a 78% chance of obtaining one statistically significant result by chance [meaning that the difference isn’t due to the vaccine], and 20% chance of having at least three such results by chance.
That said, the authors are not necessarily acting in bad faith. The shortcomings observed are related to methodological biases that are quite difficult to recognize and correct for without sufficient training and experience.
# Editor’s note:
This is known as the “multiple comparisons problem”, which arises when multiple statistical tests are done on the same set of data. This happens because every statistical test carries a risk of false positives: the more tests conducted, the more this risk is amplified, and the greater the risk of false positives. Thirty tests, which the South Korea study conducted, is a considerable number of tests.
Researchers can make corrections for multiple testing to mitigate this risk. This video from the New England Journal of Medicine explains how such corrections work.
Failing to correct for multiple comparisons can lead to false positives and incorrect conclusions. In general, any study that uses multiple statistical tests and combines positive results into a single conclusion (in this case, that COVID-19 vaccines are associated with a greater risk of cancer) should correct for multiple comparisons.
References:
- Kim et al. (2025) 1-year risks of cancers associated with COVID-19 vaccination: a large population-based cohort study in South Korea. Biomarker Research.
- Park et al. (2024) Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2021. Cancer Research and Treatment.


