- Health
The number of COVID-19 cases reported is based on a highly specific diagnostic test for COVID-19; no confusion with flu or common cold is possible
Key takeaway
Determining the spread of COVID-19 relies mainly on the detection of confirmed cases. Cases are confirmed using PCR tests which specifically detect the presence of genetic material from SARS-CoV-2, the virus responsible for COVID-19, and which do not detect viruses that cause the flu and the common cold. Therefore, even though the flu and the common cold can produce symptoms similar to a mild case of COVID-19, cases of the flu and the common cold would not be included in the reported numbers of confirmed COVID-19 cases.
Reviewed content

Verdict:
Claim:
“It's NOT a SECOND WAVE of COVID-19 coming soon. It's the NORMAL COLD / FLU SEASON”
Verdict detail
Inadequate support: The posts provide no evidence to support their assertion that COVID-19 cases reported during the fall season of 2020 are mislabeled and actually due to the common cold or flu.
Misleading: The claims rely on the faulty assumption that there is no method to distinguish COVID-19 from the common cold and the flu. In fact, COVID-19 infections are confirmed through the use of highly specific molecular tests that detect the presence of genetic material from the virus that causes COVID-19, but not the presence of other viruses such as influenza.
Full Claim
“It's NOT a SECOND WAVE of COVID-19 coming soon. It's the NORMAL COLD / FLU SEASON. Same as last year.”
Review
Claims circulated in early September 2020 stating that the common cold or flu can be mistaken for COVID-19, suggesting that current and future cases of COVID-19 should instead be attributed to common cold or flu. Posts making these claims provide no supporting evidence. They are also misleading as they leave out the important fact that COVID-19 cases are confirmed by virus-specific tests.
Firstly, the authors of these claims do not present evidence supporting their assertion that current and upcoming cases identified as COVID-19 are in fact due to the common cold of flu. Flu season commonly starts around October in the U.S., and it is likely that some cases of flu have already occurred in September 2020. This number will progressively increase as the season approaches, although data from the southern hemisphere show that the number of cases from flu is low this year, owing to social distancing and travel bans. However, no data is available that allows us to predict that these flu cases will be labeled as COVID-19. In fact, scientists interviewed by Nature think that the spread of COVID-19 may increase during the cold months of fall and winter. It is therefore possible that the cold months of fall and winter will see an increase of the number of COVID-19 cases, alongside common cold and seasonal flu.
Some symptoms of COVID-19 are distinct from those of the common cold. As Yale University indicates, COVID-19 is often associated with fatigue, shortness of breath and fever, whereas the common cold is not. On the other hand, sneezing is typical of common cold but is rare in COVID-19. However, the medical presentations of mild COVID-19 and flu are more similar and the American Society for Microbiology acknowledges that it is difficult to differentiate the two diseases based on symptoms alone.
However, the claims overlook the fact that confirmation of COVID-19 cases is based on virus-specific diagnostic tests. The U.S. Centers for Disease Control and Prevention (CDC) gathers all the results of diagnostic tests carried out by public health laboratories, clinical laboratories and commercial laboratories in the country and reports the percentage of confirmed cases. As Health Feedback explained in a previous review, confirming a case of COVID-19 depends on the detection of genetic material from the virus on the patient’s fluid by PCR. These PCR tests are specific to SARS-CoV-2 and do not detect other coronaviruses or the influenza virus, which comes from a completely different family of viruses.
The testing capacity in the U.S. steadily increased since week 16 of 2020 (mid-April) to reach a peak around week 29 (mid-July) and slightly decreased afterward. Aggregating the CDC data, Health Feedback found that laboratories carried out a total of 1,950,226 tests during week 26 (early September 2020) which returned 99,799 COVID-19 positive results (5%). Therefore, it is misleading to claim that ongoing and upcoming COVID-19 cases are due to other illnesses, given that the case confirmation is based on molecular diagnostic tests. Anticipating the overlap between the COVID-19 epidemic and the flu season, the U.S. Food and Drug Administration recently authorized a CDC-developed PCR test that can detect and distinguish both the flu virus and SARS-CoV-2.
Some versions of the claim suggest that the current epidemiological situation is similar to last year, asserting that it is normal to see more cases of respiratory illness, owing to the return of the common cold and flu season which normally takes place at the end of summer and beginning of fall. This is contradicted by data from the CDC, which registered the number of deaths per week in 2020 and compared it to the average from the previous years.
Based on these figures, we can see that August 2020 exhibited a significant amount of excess death (Figure 1). It is too early, as of 16 September 2020, to have reliable data on the number of deaths of September, as not all deaths in that month have been reported yet. However, the figure below shows that the mortality in 2020 is not “the same as last year”. In the absence of any data indicating another abnormally common cause of death in 2020, it is beyond reasonable doubt that the excess mortality is due to COVID-19 pandemic and not from the common cold and seasonal flu. If it were the case, one would expect the number of deaths to fall within the average of the previous years.
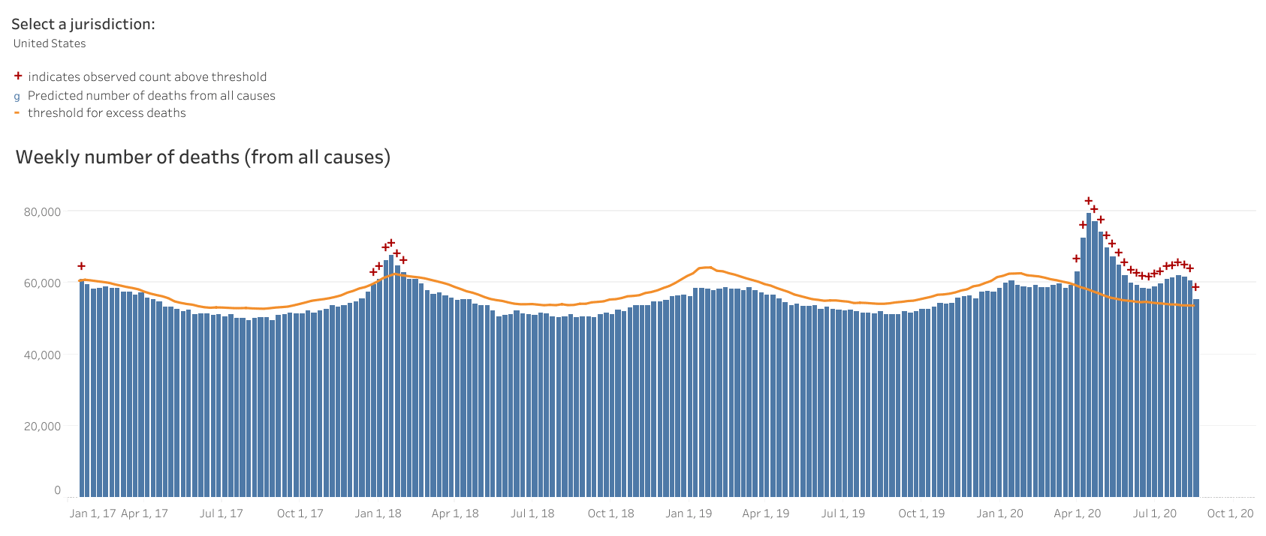
Figure 1. Deaths from all causes in the U.S. from January 2017 to August 2020. The orange line is a threshold of the expected number of deaths based on average mortality of the previous years. Deaths above the threshold (orange line) are considered “excess deaths”. Weeks where excess deaths are recorded are marked by a red cross. Data and the figure are from the U.S. CDC.
In summary, claims stating that current or upcoming cases labeled as COVID-19 are in fact due to the common cold or flu are unsupported by available evidence. They ignore the fact the number of confirmed COVID-19 cases is based on PCR tests that specifically detect the virus causing COVID-19, and thus cannot be confused with the flu infection or the common cold. It is likely that both COVID-19 and influenza will spread together during fall and winter. Although it is difficult to predict what the risk of simultaneously having both the flu and COVID-19 will be, and whether the measure of social distancing will also help reduce the flu season, experts have expressed much concern over the potential impact of having both respiratory illnesses circulating among the population at the same time.


